The FDA granted breakthrough therapy designation to pembrolizumab (Keytruda), an anti-PD-1 agent for the treatment of patients with non-small-cell lung cancer who do not have EGFR mutations or ALK rearrangements.
News
Advertisement
Stem cell therapy has gained increasing traction in various therapeutic areas, from cancer to diabetes to ocular regeneration.
Advertisement

Adding saracatinib to vascular endothelial growth factor (VEGF)-targeted therapy did not improve response rates or overall survival while adding to toxicity in VEGF-resistant metastatic renal cell carcinoma
The concept of targeting mitotic cell division to halt the progression of rapidly dividing cancer cells has long been a staple of oncology therapy, yet chemotherapy agents that are the prime examples of this approach are nonselective in their action and can kill normal and malignant cells alike.
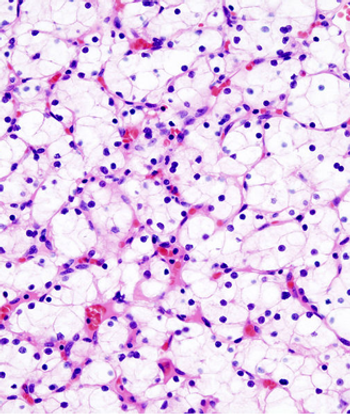
A 71-year-old woman presented with back pain and was incidentally found to have a left upper pole renal mass. She underwent left open partial nephrectomy; the pathology results revealed a 2.2-cm clear-cell renal cell carcinoma (RCC) with negative margins and a Fuhrman nuclear grade of 2.

Current novel therapeutics for the prevention and treatment of bone loss in patients with inflammatory joint disease target cytokines and other inflammatory mediators. Mesenchymal stem cell therapy is a compelling new treatment currently being studied in clinical trials.
Advertisement

A pair of medical experts – one from industry and one from academia – have teamed up to call for a new payment model for expensive gene therapies.
Bayer Healthcare and Dimension Therapeutics recently announced a partnership to advance innovative treatment options for patients with hemophilia A.
Steven A. Rosenberg, MD, PhD, discusses the implications of responses to the CAR T-cell therapy KTE-C19, particularly among patients with chemotherapy-refractory diffuse large B-cell lymphomas.

Chimeric antigen receptor T-cell therapy is an immunotherapy in which the patient's own T cells are isolated in the laboratory, redirected with a synthetic receptor to recognize a particular antigen or protein, and reinfused into the patient.
Advertisement

Immunotherapy is rapidly emerging as a very attractive and novel therapeutic approach for cancer, including for glioblastoma multiforme (GBM), the most common primary malignant brain tumor in adults.

Treatment with KTE-C19, a CD19-targeted CAR-modified T cell therapy, demonstrated an objective response rate of 92% in patients with advanced B-cell malignancies.
The treatment of inoperable stage III non–small-cell lung cancer (NSCLC) remains a challenge due to high rates of distant metastasis, local recurrence, and toxicity associated with definitive therapy.
Results of a head-to-head comparison of first-line treatment of metastatic renal cell carcinoma with the mTOR inhibitor everolimus or VEGF inhibitor sunitinib showed that everolimus did not meet noninferiority requirements as a first-line therapy.
Scientists have discovered a new molecular target for therapy to fight clear cell renal cell carcinoma, neuronal pentraxin 2 (NPTX2).
The first results from a phase I trial of gene therapy for exudative age-related macular degeneration using a subretinal injection suggest that the treatment is safe and well tolerated even in the elderly population and may eliminate the need for frequent reinjection with anti-vascular endothelial growth factor agents.
Much work is being done with Adeno-associated virus (AAV) vectors for application in retinal gene therapy, with modifications being made to the capsid and genome of the vector to generate novel variants with unique transduction profiles, according to Shannon Boye, PhD.
Lymphocyte infusions are extremely effective therapy in patients with chronic myeloid leukemia who relapse after allogeneic hematopoietic stem cell transplantation, and the timing of the infusion is relatively unimportant, according to a new study.

As gatekeepers of the cell cycle, the cyclin-dependent kinases are often implicated in the progression of cancer and make prime targets for therapy.
Researchers safely infuse engineered immune cells in groundbreaking gene therapy study.
Pfizer's deal with the French company will ensure a market share in the promising immunooncology field.

Opexa Therapeutics is initiating a phase IIb trial of a novel therapy that targets T-cells in patients with secondary progressive multiple sclerosis.
Ventana Medical Systems, Inc. and MedImmune today announced they are jointly developing a PD-L1 (SP263) immunohistochemistry assay to enroll patients in clinical trials for MedImmune's MEDI4736 anti-PD-L1 therapy for non-small cell lung carcinoma. This includes the recently commenced MEDI4736 ATLANTIC trial that will enroll only patients who express PD-L1 as determined by the VENTANA assay.
While seven drugs have been approved for clear cell renal cell carcinoma (ccRCC) since 2005, the most appropriate systemic therapy for non-clear cell renal cell carcinoma (nccRCC) is unknown.
The addition of bevacizumab to erlotinib as first-line therapy yielded a significantly extended progression-free survival in patients with advanced EGFR-mutation-positive non-small-cell lung cancer (NSCLC), according to a new phase II study.

Two patients with metastatic cervical cancer achieved durable complete responses that have so far lasted from 15 to 22 months through an adoptive T-cell therapy (ACT) targeting the human papillomavirus (HPV) in a study that researchers say supports the concept that the experimental immunotherapy approach may be beneficial in a variety of tumor types.

An interview with Renier J. Brentjens, MD, PhD, on new therapies for patients with acute and chronic leukemias, in particular novel immunotherapies such as chimeric antigen receptor T cells.

A trial (NCT01582672) that will pair a targeted treatment with a vaccine therapy for firstline treatment of renal cell carcinoma (RCC) is recruiting at the Cedars-Sinai Samuel Oschin Comprehensive Cancer Institute.
Regeneron Pharmaceuticals and Avalanche Biotechnologies announced a collaboration to discover, develop, and commercialize novel gene therapy products for the treatment of ophthalmologic diseases.
Patients with locally advanced squamous cell carcinoma of the head and neck treated with hyperfractionated radiation therapy (HFX) experienced improved local-regional control and, with patients censored at five years, improved overall survival with no increase in late toxicity.
Advertisement
Advertisement