
The FDA has approved moxetumomab pasudotox for the treatment of adult patients with relapsed or refractory hairy cell leukemia following at least 2 prior lines of therapy.
The FDA has approved moxetumomab pasudotox for the treatment of adult patients with relapsed or refractory hairy cell leukemia following at least 2 prior lines of therapy.
Antiretroviral therapy and rituximab show promise in aids-related diffuse large B-cell lymphoma patients.

Kenneth H. Shain, MD, PhD, discusses the evolution of treatment for patients with newly diagnosed multiple myeloma and how physicians are leveraging data with chimeric antigen receptor T-cell therapy and minimal residual disease negativity to improve outcomes.

Frederick L. Locke, MD, discusses the expansion of CAR T-cell therapy in patients with lymphomas following the 2017 approval of axicabtagene ciloleucel and remaining research questions with the therapy.

We headed to Tampa, Florida for a State of the Science Summit on Hematologic Malignancies. The meeting covered updates in follicular lymphoma, chronic lymphocytic leukemia, mantle cell lymphoma, multiple myeloma, acute lymphoblastic leukemia, chronic myeloid leukemia, acute myeloid leukemia, myeloproliferative neoplasms, and CAR T-cell therapy.
One patient saw a complete response, and the therapy was well tolerated, especially compared with the adverse effects sometimes seen with chimeric antigen receptor (CAR) T-cell treatment in blood cancers thus far.
Recent studies on CAR T-cell immunotherapy, and the recent approval of a new agent, add to evidence supporting the efficacy of these therapies.

The FDA has granted a fast track designation to FCX-013, a gene therapy for the treatment of patients with moderate to severe localized scleroderma.

A 17-gene signature derived from circulating tumor cells was found to correlate with response to therapy in patients with breast cancer.

David G. Maloney, MD, PhD, reviews the latest developments with chimeric antigen receptor T-cell therapy in patients with non-Hodgkin lymphoma.

The latest approach to developing a gene therapy for Duchenne muscular dystrophy shows promising results.

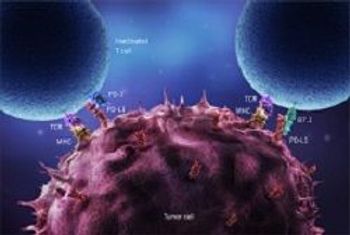
The FDA has granted a priority review for an anti-PD-1 therapy for the treatment of adults and pediatric patients with recurrent locally advanced or metastatic Merkel cell carcinoma.

Investigators in Cincinnati have linked a gene with myelodysplastic syndromes, potentially offering the first step toward a new genetic therapy.
Only 1 day after the European Commission approved CAR T-cell therapies, the National Institute for Health and Care Excellence deemed the treatment too expensive to justify on Britain's state-funded health service.

The FDA has granted an orphan drug designation to ReflectionBio's AAV-based gene therapy, the RBIO-101 program (AAV.CYP4V2), for the treatment of Bietti's crystalline dystrophy (BCD).

Every week, The American Journal of Managed Care® recaps the top managed care news of the week, and you can now listen to it on our podcast, Managed Care Cast.
Jonathon B. Cohen, MD, discusses the potential benefit of offering deferred therapy to asymptomatic patients with mantle cell lymphoma.

The FDA grants an orphan drug designation to a novel gene therapy candidate for the treatment of patients with hereditary angioedema.

The first patient has been treated in a phase 2b dose-confirmation study of AMT-061, an investigational gene therapy for the treatment of patients with severe and moderately severe hemophilia B. Once the dosing of AMT-061 is confirmed, the safety and efficacy of the therapy will be evaluated in the global phase 3 HOPE-B clinical trial.

The mesenchymal stem cell therapy passed an interim safety analysis for the first 31 patients with amyotrophic lateral sclerosis.
During a meeting of the Medicare Evidence Development and Coverage Advisory Committee (MEDCAC), panelists heard from chimeric antigen receptor (CAR) T therapy drug makers, health researchers, and policy makers, and mostly endorsed including patient-reported outcomes (PROs) in its final national coverage analysis decision, expected next year.

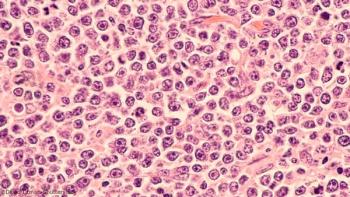
A blood test that tracks the rise and fall of circulating tumor DNA (ctDNA) levels can predict how patients with diffuse large B-cell lymphoma will respond to therapy within days of starting treatment.

Axicabtagene ciloleucel (axi-cel; Yescarta) is being evaluated in patients with relapsed or refractory mantle cell lymphoma—a rare B-cell non-Hodgkin lymphoma that contributes 4200 new patients in the United States each year.

The designation is backed by positive interim data from ASPIRO, which has demonstrated significant improvements in neuromuscular and respiratory function at week 24.
The first chimeric antigen receptor (CAR) T-cell therapy was approved just a year ago, changing the face of treatment for certain types of leukemias and lymphomas but carrying with it the downsides of toxicity and cost. A year later, scientists from a major cancer center said that they’ve made headway to discovering more about the T-cell signaling patterns and that understanding more about the biological pathways could help design the next generation of CAR-T treatments.

The FDA has granted a fast track designation to gene therapy product candidate AAV-CNGB3 for the treatment of achromatopsia caused by mutations in the CNGB3 gene.

The FDA has approved Bristol-Meyers Squibb Company’s nivolumab (Opdivo) for the treatment of metastatic small cell lung cancer (SCLC) that has progressed after platinum-based chemotherapy and at least 1 other line of therapy.

The FDA has approved single-agent nivolumab for the treatment of patients with small cell lung cancer with disease progression following 2 or more lines of therapy.
Next week, a CMS committee will hold a day-long meeting to discuss a national coverage determination (NCD) for chimeric antigen receptor (CAR) T-cell immunotherapies, and in Thursday’s New England Journal of Medicine, Peter B. Bach, MD, MAPP, reviewed several strategies open to CMS as it continues to try to determine how to pay for CAR T.

The FDA will start to review gene therapy experiments and products the same as other treatments and drugs; Alaska and Minnesota have become models for other states looking to curb health insurance premium increases with reinsurance programs; patients with limited English proficiency often have to rely on family members and friends to interpret for them, which can have serious consequences.